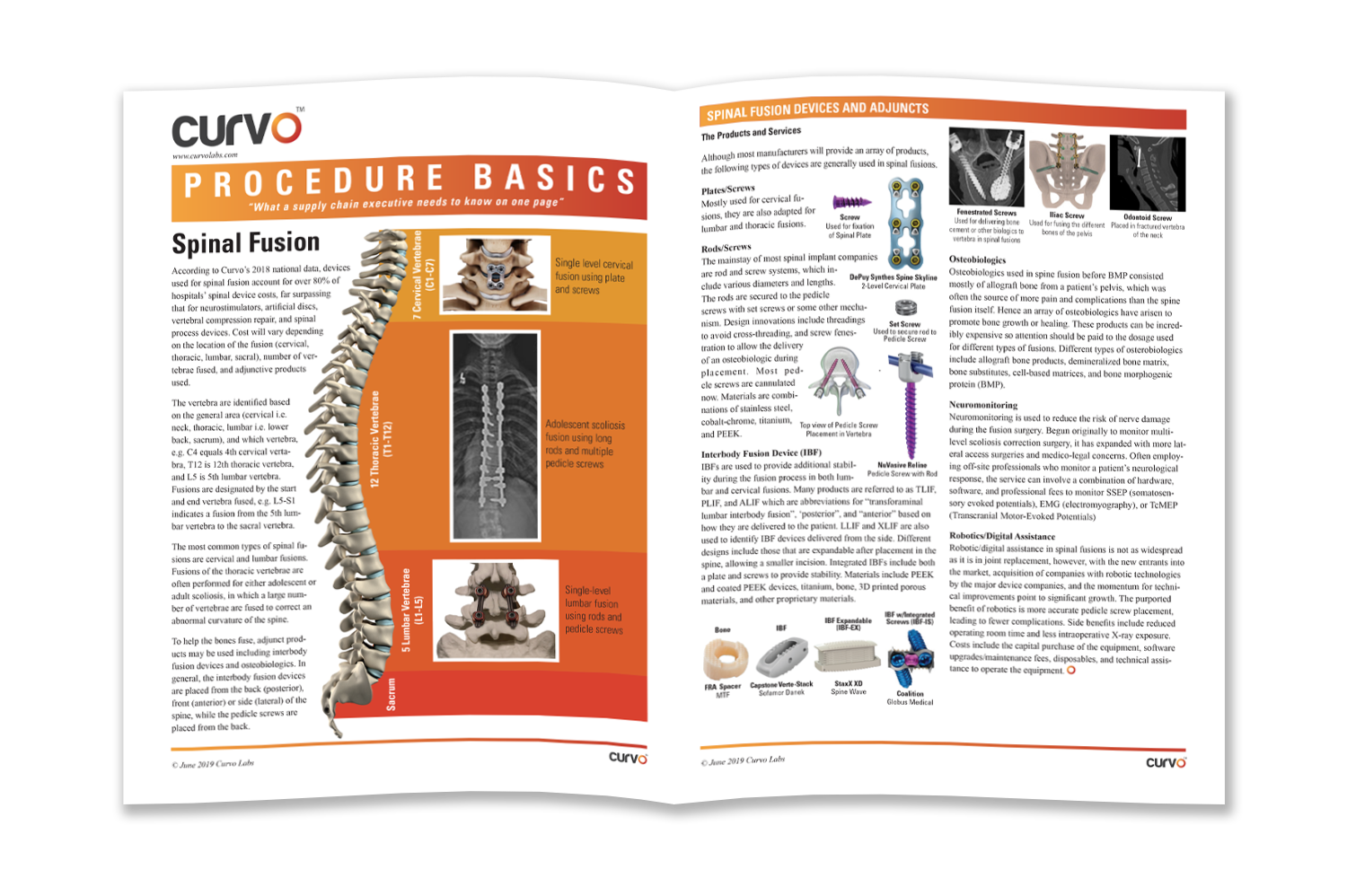
According to Curvo’s 2018 national data, devices used for spinal fusion accounted for over 80% of hospitals’ spinal device costs, far surpassing that for neurostimulators, artificial discs, vertebral compression repair, and spinal process devices. Cost will vary depending on the location of the fusion (cervical, thoracic, lumbar, sacral), number of vertebrae fused, and adjunctive products used.
The vertebra are identified based on the general area (cervical i.e. neck, thoracic, lumbar i.e. lower back, sacrum), and which vertebra, e.g. C4 equals 4th cervical vertebra, T12 is 12th thoracic vertebra, and L5 is 5th lumbar vertebra. Fusions are designated by the start and end vertebrae fused, e.g. L5-S1 indicates a fusion from the 5th lumbar vertebra to the sacral vertebra.
Most Common Types of Spinal Fusions
The most common types of spinal fusions are cervical and lumbar fusions. Fusions of the thoracic vertebrae are often performed for either adolescent or adult scoliosis, in which a large number of vertebrae are fused to correct an abnormal curvature of the spine.
To help the bones fuse, adjunct products may be used including interbody fusion devices and osteobiologics. In general, the interbody fusion devices are placed from the back (posterior), front (anterior) or side (lateral) of the spine, while the pedicle screws are placed from the back.
Products and Services Used in Spinal Fusion Procedures
Although most manufacturers will provide an array of products, the following types of devices are generally used in spinal fusions.
Plates/Screws
Mostly used for cervical fusions, they are also adapted for lumbar and thoracic fusions.
Rods/Screws
The mainstay of most spinal implant companies are rod and screw systems, which include various diameters and lengths. The rods are secured to the pedicle screws with set screws or some other mechanism. Design innovations include threadings to avoid cross-threading, and screw fenestration to allow the delivery of an osteobiologic during placement. Most pedicle screws are cannulated now. Materials are combinations of stainless steel, cobalt-chrome, titanium, and PEEK.
Interbody Fusion Device (IBF)
IBFs are used to provide additional stability during the fusion process in both lumbar and cervical fusions. Many products are referred to as TLIF, PLIF, and ALIF which are abbreviations for “transforaminal lumbar interbody fusion”, "posterior”, and “anterior” based on how they are delivered to the patient. LLIF and XLIF are also used to identify IBF devices delivered from the side. Different designs include those that are expandable after placement in the spine, allowing a smaller incision. Integrated IBFs include both a plate and screws to provide stability. Materials include PEEK and coated PEEK devices, titanium, bone, 3D printed porous materials, and other proprietary materials.
Osteobiologics
Osteobiologics used in spine fusion before BMP consisted mostly of allograft bone from a patient’s pelvis, which was often the source of more pain and complications than the spine fusion itself. Hence an array of osteobiologics have arisen to promote bone growth or healing. These products can be incredibly expensive so attention should be paid to the dosage used for different types of fusions. Different types of osteobiologics include allograft bone products, demineralized bone matrix, bone substitutes, cell-based matrices, and bone morphogenic protein (BMP).
Neuromonitoring
Neuromonitoring is used to reduce the risk of nerve damage during the fusion surgery. Begun originally to monitor multi-level scoliosis correction surgery, it has expanded with more lateral access surgeries and medico-legal concerns. Often employing off-site professionals who monitor a patient’s neurological response, the service can involve a combination of hardware, software, and professional fees to monitor SSEP (somatosensory evoked potentials), EMG (electromyography), or TcMEP (Transcranial Motor-Evoked Potentials)
Robotics/Digital Assistance
Robotic/digital assistance in spinal fusions is not as widespread as it is in joint replacement, however, with the new entrants into the market, acquisition of companies with robotic technologies by the major device companies, and the momentum for technical improvements point to significant growth. The purported benefit of robotics is more accurate pedicle screw placement, leading to fewer complications. Side benefits include reduced operating room time and less intraoperative X-ray exposure. Costs include the capital purchase of the equipment, software upgrades/maintenance fees, disposables, and technical assistance to operate the equipment.
Get the full Procedure Brief on Spinal Fusion Devices and Procedure Basics.
